Efectividad del ketoconazol oral en el tratamiento de la dermatitis seborreica moderada a grave
Palabras clave:
ketoconazol, dermatitis seborreica, efectividad, dermatologíaResumen
Introducción: La dermatitis seborreica es una enfermedad inflamatoria cró- nica de difícil manejo, que puede afectar diferentes zonas anatómicas. Su tratamiento con derivados imidazólicos, como el ketoconazol, produce resultados variables que dependen tanto de la seriedad y extensión de las lesiones como de la vía de administración del medicamento. El ketoconazol oral ha sido el tratamiento de elección en el manejo de la dermatitis seborreica moderada a grave en el Centro Dermatológico Federico Lleras Acosta; sin embargo, no existen estudios clínicos en Colombia que hayan evaluado su efectividad. El objetivo del presente estudio fue establecer la efectividad del ketoconazol oral en casos de dermatitis seborreica moderada a grave, comparando el compromiso clínico antes del tratamiento y después de él.
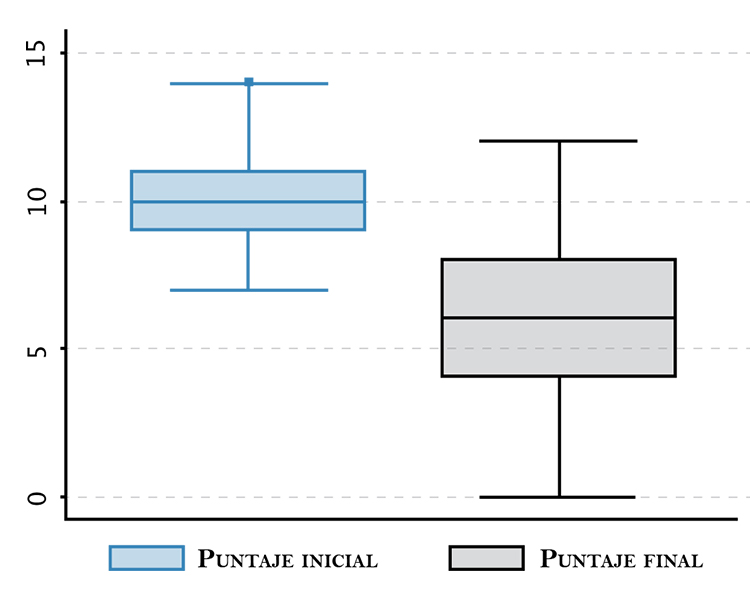
Materiales y métodos: Se llevó a cabo un estudio clínico seudoexperimental para evaluar la efectividad de un ciclo de tratamiento con 200 mg diarios de ketoconazol durante treinta días. Se incluyeron 96 pacientes con diagnóstico de dermatitis seborreica moderada a grave, que aceptaron participar en el estudio siguiendo los principios de buenas prácticas clínicas. Para establecer el grado de compromiso, se utilizó la escala de gravedad de dermatitis seborreica de la guía de práctica clínica del Centro Dermatológico Federico Lleras Acosta. Esta escala incluye el grado de descamación, la presencia de prurito y eritema, y la localización anatómica. Los valores se establecen en un rango de 0 a 100, donde 100 es el nivel de compromiso máximo. Se incluyeron pacientes con puntuaciones iguales o superiores a 50, punto de corte para establecer el compromiso moderado. Se consideraron casos graves los que obtuvieron valores superiores a 75 puntos. El porcentaje de mejoría obtenido se calculó a partir de la diferencia entre el grado de compromiso inicial y el compromiso al final del ciclo. Un tratamiento fue considerado efectivo cuando la mejoría obtenida al final del tratamiento fue igual al 70% o mayor.
Resultados: Ochenta y seis sujetos finalizaron el estudio, con un porcentaje de pérdidas en el seguimiento de 11%. La media de compromiso al ingreso fue de 67 puntos y al terminar el ciclo de tratamiento, de 33 puntos. Se establecieron diferencias significativas en las medias antes del tratamiento y después de él (p=0,001). El 48% (IC95 %: 37-58) de los sujetos alcanzaron un porcentaje de mejoría clínica igual al 70% o mayor. Se presentaron efectos secundarios en 11 pacientes (12,8%; IC95 %: 6,5-21,7), definidos como leves y de resolución espontánea.
Conclusiones: El ketoconazol oral es una alternativa terapéutica en el tratamiento de pacientes con dermatitis seborreica moderada a grave, con un perfil de seguridad adecuado a las dosis utilizadas y durante el tiempo establecido en este estudio.
Biografía del autor/a
Camilo Andrés Morales
Médico dermatólogo, Oficina de Docencia e Investigación, Centro Dermatológico Federico Lleras Acosta, E.S.E., Bogotá, D.C., Colombia
Guillermo Sánchez
Médico epidemiólogo, M.Sc. en Epidemiología Clínica, Oficina de Docencia e Investigación, Centro Dermatológico Federico Lleras Acosta, E.S.E., Bogotá, D.C., Colombia
Referencias bibliográficas
2. Schwartz RA, Janusz CA, Janniger CK. Seborrheic dermatitis: an overview. Am Fam Physician. 2006;74:125-30.
3. Borgers M, Degreef H. The role of ketoconazole in seborrheic dermatitis. Cutis. 2007;80:359-63.
4. Gupta AK, Nicol K, Batra R. Role of antifungal agents in the treatment of seborrheic dermatitis. Am J Clin Dermatol. 2004;5:417-22.
5. Faergemann J, Borgers M, Degreef H. A new ketoconazole topical gel formulation in seborrhoeic dermatitis: an updated review of the mechanism. Expert Opin Pharmacother. 2007;8:1365-71.
6. Faergemann J. In vitro and in vivo activities of ketoconazole and itraconazole against Pityrosporum orbiculare. Antimicrob Agents Chemother. 1984;26:773-4.
7. Strippoli V, Piacentini A, D’Auria FD, Simonetti N. Antifungal activity of ketoconazole and other azoles against Malassezia furfur in vitro and in vivo. Infection. 1997;25:303-6.
8. van Cutsem J, van Gerven F, Cauwenbergh G, Odds F, Janssen PA. The antiinflammatory effects of ketoconazole. A comparative study with hydrocortisone acetate in a model using living and killed Staphylococcus aureus on the skin of guineapigs. J Am Acad Dermatol. 1991;25:257-61.
9. Hegemann L, Toso SM, Lahijani KI, Webster GF, Uitto J. Direct interaction of antifungal azole-derivatives with calmodulin: a possible mechanism for their therapeutic activity. J Invest Dermatol. 1993;100:343-6.
10. Farr PM, Krause LB, Marks JM, Shuster S. Response of scalp psoriasis to oral ketoconazole. Lancet. 1985;2:921-2.
11. Sohnle PG, Collins-Lech C. Activation of complement by Pityrosporum orbiculare. J Invest Dermatol. 1983;80:93-7.
12. Shuster S. The aetiology of dandruff and the mode of action of therapeutic agents. Br J Dermatol. 1984;111:235-42.
13. Ackerman AB, Kligman AM. Some observations on dandruff. J Soc Cosmet Chem. 1967;20:81-101.
14. Leyden JJ, McGinley KJ, Kligman AM. Role of microorganisms in dandruff. Arch Dermatol. 1976;112:333-8.
15. Alexander S. Do shampoos affect dandruff ? Br J Dermatol. 1967;79:92-5.
16. Aron-Brunetiere R, Dompmartin-Pernot D, Drouhet E. Treatment of pityriasis capitis (dandruff) with econazole nitrate. Acta Derm Venereol. 1977;57:77-80.
17. Ro BI, Dawson TL. The role of sebaceous gland activity and scalp microfloral metabolism in the etiology of seborrheic dermatitis and dandruff. J Investig Dermatol Symp Proc. 2005;10:194-7.
18. Pierard-Franchimont C, Hermanns JF, Degreef H, Pierard GE. From axioms to new insights into dandruff. Dermatology. 2000;200:93-8.
19. Gupta AK, Bluhm R, Cooper EA, Summerbell RC, Batra R. Seborrheic dermatitis. Dermatol Clin. 2003;21:401-12.
20. Machin D, Campbell MJ. Statistical tables for the design of clinical trials. Oxford, St. Louis: Blackwell Scientific Publications; 1987.
21. Ministerio de Salud. Resolución N° 008430 de 1993: normas científicas, técnicas y administrativas para la investigación en salud; 1993. Fecha de consulta: 19 de julio de 2010. Disponible en: http://201.234.78.165:8080/portalcol/downloads/ archivosSoporteConvocatorias/751.pdf.
22. World Health Organization. WHO drug information. Current topics: Declaration of Helsinki and placebo-controlled clinical trials. Geneva: World Health Organization; 2001. Fecha de consulta: 19 de julio de 2010. Disponible en: http:// apps.who.int/medicinedocs/pdf/h2989e/h2989e.pdf.
23. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects; 2001. Fecha de consulta: 19 de julio de 2010. Disponible en: http://www.wma.net/ en/30publications/10policies/b3/17c.pdf.
24. McGrath J, Murphy GM. The control of seborrhoeic dermatitis and dandruff by antipityrosporal drugs. Drugs. 1991;41:178-84.
25. Faergemann J, Jones JC, Hettler O, Loria Y. Pityrosporum ovale (Malassezia furfur) as the causative agent of seborrhoeic dermatitis: new treatment options. Br J Dermatol. 1996;134:12-5.
26. Bergbrant IM. Seborrhoeic dermatitis and Pityrosporum yeasts. Curr Top Med Mycol. 1995;6:95-112.
27. Sei Y, Hamaguchi T, Ninomiya J, Nakabayashi A, Takiuchi I. Seborrhoeic dermatitis: treatment with anti-mycotic agents. J Dermatol. 1994;21:334-40.
28. van Cutsem J, van Gerven F, Fransen J, Schrooten P, Janssen PA. The in vitro antifungal activity of ketoconazole, zinc pyrithione, and selenium sulfide against Pityrosporum and their efficacy as a shampoo in the treatment of experimental pityrosporosis in guinea pigs. J Am Acad Dermatol. 1990;22:993-8.
29. Farr PM, Shuster S. Treatment of seborrhoeic dermatitis with topical ketoconazole. Lancet. 1984;2:1271-2.
30. Pierard-Franchimont C, Pierard GE, Arrese JE, De Doncker P. Effect of ketoconazole 1% and 2% shampoos on severe dandruff and seborrhoeic dermatitis: clinical, squamometric and mycological assessments. Dermatology. 2001;202:171-6.
31. Peter RU, Richarz-Barthauer U. Successful treatment and prophylaxis of scalp seborrhoeic dermatitis and dandruff with 2% ketoconazole shampoo: results of a multicentre, double-blind, placebo-controlled trial. Br J Dermatol. 1995;132:441-5.
32. Green CA, Farr PM, Shuster S. Treatment of seborrhoeic dermatitis with ketoconazole. II. Response of seborrhoeic dermatitis of the face, scalp and trunk to topical ketoconazole. Br J Dermatol. 1987;116:217-21.
33. Elewski B, Ling MR, Phillips TJ. Efficacy and safety of a new once-daily topical ketoconazole 2% gel in the treatment of seborrheic dermatitis: a phase III trial. J Drugs Dermatol. 2006;5:646-50.
34. Zienicke H, Korting HC, Braun-Falco O, Effendy I, Hagedorn M, Kuchmeister B, et al. Comparative efficacy and safety of bifonazole 1% cream and the corresponding base preparation in the treatment of seborrhoeic dermatitis. Mycoses. 1993;36:325-31.
35. Dupuy P, Maurette C, Amoric JC, Chosidow O. Randomized, placebo-controlled, double-blind study on clinical efficacy of ciclopiroxolamine 1% cream in facial seborrhoeic dermatitis. Br J Dermatol. 2001;144:1033-7.
36. Pierard-Franchimont C, Goffin V, Decroix J, Pierard GE. A multicenter randomized trial of ketoconazole 2% and zinc pyrithione 1% shampoos in severe dandruff and seborrheic dermatitis. Skin Pharmacol Appl Skin Physiol. 2002;15:434-41.
37. Dreno B, Chosidow O, Revuz J, Moyse D. Lithium gluconate 8% vs ketoconazole 2% in the treatment of seborrhoeic dermatitis: a multicentre, randomized study. Br J Dermatol. 2003;148:1230-6.
38. Chosidow O, Maurette C, Dupuy P. Randomized, openlabeled, non-inferiority study between ciclopiroxolamine 1% cream and ketoconazole 2% foaming gel in mild to moderate facial seborrheic dermatitis. Dermatology. 2003;206:233-40.
39. Shuster S, Meynadier J, Kerl H, Nolting S. Treatment and prophylaxis of seborrheic dermatitis of the scalp with antipityrosporal 1% ciclopirox shampoo. Arch Dermatol. 2005;141:47-52.
40. Elewski BE, Abramovits W, Kempers S, Schlessinger J, Rosen T, Gupta AK, et al. A novel foam formulation of ketoconazole 2% for the treatment of seborrheic dermatitis on multiple body regions. J Drugs Dermatol. 2007;6:1001-8.
41. Ford GP, Farr PM, Ive FA, Shuster S. The response of seborrhoeic dermatitis to ketoconazole. Br J Dermatol. 1984;111:603-7.
42. Hjorth N, Clemmensen OJ. Treatment of dermatitis of the head and neck with ketoconazole in patients with type I hypersensitivity for Pityrosporum orbiculare. Semin Dermatol. 1983;2:26-9.
43. Rosenberg EW, Belew PW. Improvement of psoriasis of the scalp with ketoconazole. Arch Dermatol. 1982;118:370-1.
44. Wishner AJ, Teplitz ED, Goodman DS. Pityrosporum, ketoconazole, and seborrheic dermatitis. J Am Acad Dermatol. 1987;17:140-1.
45. Baysal V, Yildirim M, Ozcanli C, Ceyhan AM. Itraconazole in the treatment of seborrheic dermatitis: a new treatment modality. Int J Dermatol. 2004;43:63-6.
46. Vena GA, Micali G, Santoianni P, Cassano N, Peruzzi E. Oral terbinafine in the treatment of multi-site seborrhoic dermatitis: a multicenter, double-blind placebo-controlled study. Int J Immunopathol Pharmacol. 2005;18:745-53.
47. Kose O, Erbil H, Gur AR. Oral itraconazole for the treatment of seborrhoeic dermatitis: an open, noncomparative trial. J Eur Acad Dermatol Venereol. 2005;19:172-5.
48. Zisova LG. Fluconazole and its place in the treatment of seborrheic dermatitis-new therapeutic possibilities. Folia Med (Plovdiv). 2006;48:39-45.
49. Pierard GE, Ausma J, Henry F, Vroome V, Wouters L, Borgers M, et al. A pilot study on seborrheic dermatitis using pramiconazole as a potent oral anti-Malassezia agent. Dermatology. 2007;214:162-9.
50. Shemer A, Kaplan B, Nathansohn N, Grunwald MH, Amichai B, Trau H. Treatment of moderate to severe facial seborrheic dermatitis with itraconazole: an open non-comparative study. Isr Med Assoc J. 2008;10:417-8.
51. Park HS, Chong HW, Lee YW, Huh CH, Lee HI, Kim BJ, Kim MN. A study upon parameters useful for evaluating the antidandruff efficacy of 1% zinc pyrithione shampoo. Int J Trichol. 2009;1:60-1.
52. Leyden JJ MK, Kligman AM. Shorter methods for evaluating antidandruff agents. J Soc Cosmet Chem. 1975;26:573-80.
53. Piérard Franchimont C, Uhoda E, Loussouarn G, Saint Léger D, Piérard G. Effect of residence time on the efficacy of antidandruff shampoos. Int J Cosmet Sci. 2003;25:267-71.
54. Lewis JH, Zimmerman HJ, Benson GD, Ishak KG. Hepatic injury associated with ketoconazole therapy. Analysis of 33 cases. Gastroenterology. 1984;86:503-13.
55. Janssen PA, Symoens JE. Hepatic reactions during ketoconazole treatment. Am J Med. 1983;74:80-5.
56. Stricker BH, Blok AP, Bronkhorst FB, van Parys GE, Desmet VJ. Ketoconazole-associated hepatic injury. A clinicopathological study of 55 cases. J Hepatol. 1986;3:399-406. 5
7. Bercoff E, Bernuau J, Degott C, Kalis B, Lemaire A, Tilly H, et al. Ketoconazole-induced fulminant hepatitis. Gut. 1985;26:636-8.
58. Findor JA, Sorda JA, Igartua EB, Avagnina A. Ketoconazoleinduced liver damage. Medicina (B Aires). 1998;58:277-81.
59. Chien RN, Sheen IS, Liaw YF. Unintentional rechallenge resulting in a causative relationship between ketoconazole and acute liver injury. Int J Clin Pract. 2003;57:829-30.
60. van Parys G, Evenepoel C, van Damme B, Desmet VJ. Ketoconazole-induced hepatitis: a case with a definite cause-effect relationship. Liver. 1987;7:27-30.
61. Duarte PA, Chow CC, Simmons F, Ruskin J. Fatal hepatitis associated with ketoconazole therapy. Arch Intern Med. 1984;144:1069-70.
62. Klausner MA. Ketoconazole and hepatitis. J Am Acad Dermatol. 1992;26:1028-30.
63. Garcia-Rodriguez LA, Duque A, Castellsague J, PerezGutthann S, Stricker BH. A cohort study on the risk of acute liver injury among users of ketoconazole and other antifungal drugs. Br J Clin Pharmacol. 1999;48:847-52.
64. Chien RN, Yang LJ, Lin PY, Liaw YF. Hepatic injury during ketoconazole therapy in patients with onychomycosis: a controlled cohort study. Hepatology. 1997;25:103-7.
Cómo citar
Descargas
Descargas
Publicado
Cómo citar
Número
Sección

| Estadísticas de artículo | |
|---|---|
| Vistas de resúmenes | |
| Vistas de PDF | |
| Descargas de PDF | |
| Vistas de HTML | |
| Otras vistas | |