Inmunología y terapia biológica en psoriasis
Palabras clave:
Psoriasis, terapia biológica, tratamientoResumen
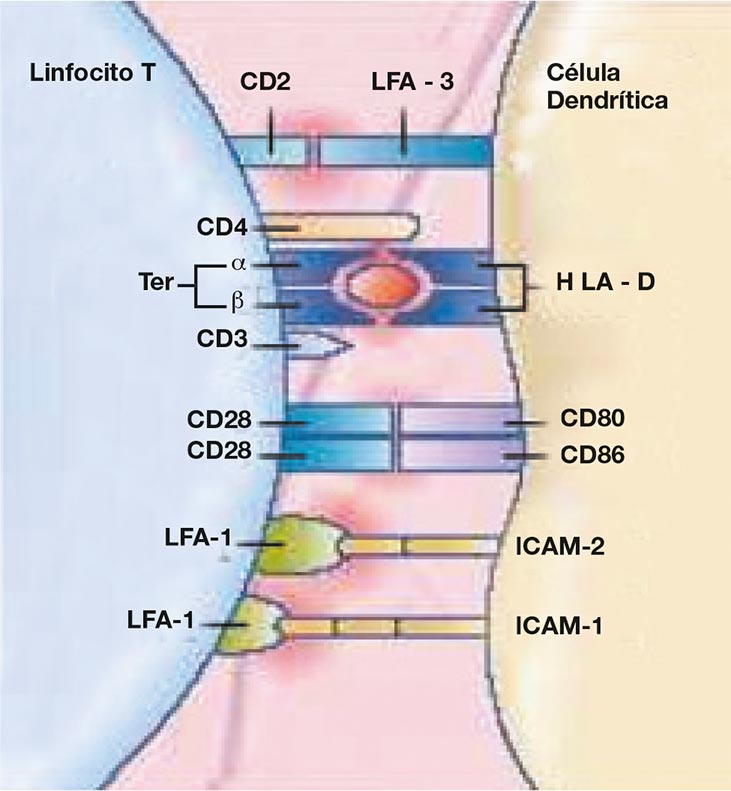
LA PSORIASIS es una enfermedad inflamatoria de la piel, donde ocurren complejas interacciones entre genes susceptibles, mecanismos efectores inmunológicos y desencadenantes ambientales, lo que produce una alteración en el recambio celular que resulta en una diferenciación terminal anormal de los queratinocitos, asociado a un deterioro de la función de barrera epidérmica.
El conocimiento de la inmuno-patogénesis de la enfermedad se ha convertido en el blanco de los esfuerzos para encontrar una terapia específica con pocos efectos adversos y un buen margen de seguridad.
Gracias a la biotecnología y al uso de la ingeniería genética ha sido posible el desarrollo de la terapia biológica, la cual comprende proteínas con actividad farmacológica que intervienen en los diferentes procesos de la fisiopatología de la enfermedad. Aunque los agentes biológicos son relativamente nuevos en dermatología tienen una larga historia de uso en otras áreas de la medicina.
El objetivo de este artículo es revisar la fisiopatogenia de la enfermedad y la aplicación y uso de los agentes biológicos modificadores de la misma.
Biografía del autor/a
Dora Luz Fonseca
RIII Dermatología, Universidad Militar Nueva Granada, Bogotá
Liliana Aristizábal
RIII Dermatología, Universidad Militar Nueva Granada, Bogotá.
Claudia Cruz
RII Dermatología, Universidad Militar Nueva Granada, Bogotá.
Liliana Herrera
RI Dermatología, Universidad Militar Nueva Granada, Bogotá.
Johana Prada
RI Dermatología, Universidad Militar Nueva Granada, Bogotá.
Guillermo De la Cruz
RI Dermatología, Universidad Militar Nueva Granada, Bogotá.
Olga Parra
RII Dermatología, Universidad Militar Nueva Granada, Bogotá.
Ximena Sánchez
Especialista Dermatóloga, Hospital Militar Central Bogotá.
César González
Especialista Dermatólogo agregado, Hospital Militar Central, Bogotá.
Luis Castro
Especialista Inmuno-dermatólogo, Clínica Mayo, USA, Dermatólogo Hospital Militar Central, Bogotá.
Referencias bibliográficas
2. Sobell J. Overview of biologic agents in medicine and dermatology.. Semin cutan Med surg. 2005; 24: 2 -9.
3. Bowcock AM, Barker JN. Genetics of psoriasis: the potential impacts on new therapies. J Am Acad Dermatol. 2003; 49 (Suppl) S51-6.
4. Krueger G. Psoriasis-recent advances in understanding its pathogenesis and treatment. J Am Acad Dermatol. 2005;53, 1: S94-S100
5. Gaspari A. Innate and adaptive immunity an d the pathophysiology of psorisis. J Am Acad dermatol. 2006.54: S67-80
6. Nickoloff BJ. The immunologic and genetic basis of psoriasis. Arch Dermatol 1999; 135:1104- 10.
7. Griffi ths C. The immunological basis of Psoriasis. JEADV, 2003: 17, S2: 1-5.
8. Mehlis SL, Gordon KB. The immunology of psoriasis and biologic immutherapy. J Am Acad Dermatol. 2003; 49: S44-50.
9. Lebwohl M. Psoriasis. Lancet 2003; 361: 1197-204.
10. Guenther LC, Ortonne JP. Pathophysiology of psoriasis: science venid therapy. J Cutan Med Surg 2002;6 (S 3):2-7.
11. Lee RE, Gaspari AA, Lotze MT., et al. Interleukin 2 and psoriasis. Arch Dermatol 1988; 124:1811-5.
12. Chaturvesi V, Qin J, Denning MF et al. Apoptosis in proliferating senescent, and immortalized Keratinocytes. J. Biol Chem 1999; 274: 23358-67.
13. Gottlieb AB. TNF-alpha and apoptosis: implications for the pathogenesis and treatment of psoriasis. J Drugs Dermatol. 2002; 1:264-75.
14. Gofee B, Cather JC. Etanercept: an overview. J Am Acad Dermatol 2003; 49:S105-11
15. McKay, IA. Leigh, IM. Altered Keratinocyto growth and Differentiation in psoriasis. Clin Dermatol 1995; 13: 105-14.
16. Barrer JN, Mitra RS, Griffi ths CEM., et al. Keratinocytes as initators of infl ammation. Lancet 1991; 337: 211-4.
17. Krueger GG, Bergstresser PR, Lowe NJ., et al. Psorisis. J Am Acad Dermatol 1984; 11: 937-47.
18. Pias EK, Vargas J, Diaz LA. Humoral autoinmunity in pemphigus. Autoinmunity 2004;37:283- 47.
19. Feldam S. Decisión points for the initiation of systemic treatment for psoriasis. J Am Acad Dermatol. 2005;53:101- 07.
20. Koo J, Khera P. Update on the mechanisms and effi cacy of biological therapies for psoriasis. J of dermatol scien; 2005,38: 75-87.
21. Thomas VD, Yang C, Kvedar J. Biologics in psoriasis: A quick reference guide. J Am Acad Dermatol; 2005, 53: 346- 51.
22. Kipnis C, Myers W, Opeola M., et al. Biologic treatments for psoriasis. J Am Acad Dermatol. 2005; 52:671- 82.
23. Lebwolhl M, Christophers E, Langley R., et al. An international, randomized, double-blind, placebo-controlled phase 3 trial of intramuscular alefacept in patients with chronic plaque psoriasis. Arch dermatol; 2003. 139: 719-27.
24. Finlay A, Salek M, Haney J. Intramuscular alefacept improves health-related quality of life in patients with chronic plaque psoriasis. J Am Acad Dermatol. 2003, 206:307-15.
25. Kraan M, Van Kujik A, Dinant HJ., et al. Alefacept treatment in psoriatic arthritis: reduction of the effector T cell population in peripheral blood and synovial tissue with improvement of clinical signs of arthritis. Arthritis Rheum; 2002. 46:2776-84.
26. Carey, W. Relapse, rebound and psoriasis adverse events: An advisory group report. J Am Acad Dermatol. 2006;54: S171-81.
27. Menter, A. Long-term management of plaque psoriasis with continuous efalizumab therapy. J Am Acad Dermatol. 2006;54: S182- 8.
28. Leonardi, C. Current concepts and review of efalizumab in the treatment of psoriasis. Dermatol Clin. 2004; 22: 427-35.
29. Gordon K, Papp KA, Hamilton TK, et al. Efalizumab for patients with moderate to severe plaque psoriasis a randomized controlled trial. JAMA; 2003. 290:3073-80.
30. Gottlieb A. Long-term continuous efalizumab therapy in patients with moderate to severe chronic plaque psoriasis: Update results from an ongoing trial. J Am Acad Dermatol. 2006;54:S154- 63.
31. Papp K. Efalizumab retreatment in patients with moderate to severe chronic plaque psoriasis. J Am Acad Dermatol. 2006; 54: S164- 70.
32. Lebwohl M, Tyring SK, Hamilton TK, et al. A novel targeted T cell modulator, efalizumab, for plaque psoriasis. N Engl J Med. 2003. 349: 2004-13.
33. Gottlieb AB, Krueguer JG Bright R, et al. Effects of administration of single dose of a humanized monoclonal antibody to CD11a on the inmunobiology and clinical activity of psoriasis. J Am Acad Dermatol; 2000. 42: 428-35.
34. Goldsmith D, Wagstaff A. Etarnecept: a review of its use in the management of plaque psoriasis and psoriatic arthritis. Am Clin dermatol. 2005; 6: 121- 36.
35. Kirby B, Griffi ths C. Novel immune –based therapies for psoriasis. Br J dermatol. 2002; 146: 246-551.
36. Glottlieb AB. Clinical research helps elucidate the role of tumor necrosis factor alfa in the pathogenesis of T1 mediate immune disorders: use of targert immunotherapeutics as pathogenic probes. Lupus. 2003; 12: 190- 94.
37. Papp K, Tyring S, Prinz J. A global phase III randomized controlled trial of etanercept in psoriasis: safety, effi cacy, and effect of dose reduction. Br J Dermatol. 2005; 152:1304– 12.
38. Leonardi CL, Powers JL, Matheson RT, et al. Etanercept as monoterapy in patients with psoriasis. N Engl Med. 2003;349: 2014-22.
39. Gottlieb AB, Matheson RT, Lowe N, et al. A Randomized trial of etanercept as monoterapy for psoriasis. Arch Dermatol, 2003; 139: 1627-32.
40. Mease PJ, Goffe BS, Metz J, et al. Etanercept in the treatment of psoriatic arthritis and psoriasis: a randomized trial. Lancet. 2000; 356: 385-90.
41. Esposito M, Mazzotta A, De Felice C, et al. Treatment of erythrodermic psoriasis with etanercept. Br J Dermatol. 2006; 155: 156-59.
42. Markham T, Mulla R, Golden-Mason L, et al. Resolution of endothelial activation and down-regulation of Tie 2 receptor in psoriatic skin after infl iximab therapy.. J Am Acad Dermatol. 2006; 54: 1003-12.
43. Menter A, Feldman S, Weinstein G., et al. A randomized comparison of continuous vs intermittent infl iximab maintenance regimens over 1 year in the treatment of moderate to severe plaque psoriasis. J Am Acad Dermatol. 2007; 56:31e1- 5.
44. Gottlieth, A. Infl iximab for psoriasis. J Am Acad Dermatol 2003; 49: s112 -7.
45. Chaudhari U, Romano P, Mulcahey LD, et al. Effi cacy and safety of infl iximab monotherapy for plaque type psoriasis: a randomized trial. Lancet. 2001; 357: 1842-7.
46. Gottlieb A, Ramamurthi R, Romano P, et al. Pharmacodynamic and pharmacokinetic response to anti-tumor necrosis factor alpha monoclonal antibody, infl iximab, treatment of moderate to severe psoriasis vulgaris. J Am Acad Dermatol. 2003; 48:68-75.
47. Rycle L, Kruithor E, Van Damme N, et al. Antinuclear antibodies following infl iximab treatment in patients with rheumatoid arthritis or spondylarthropaty. Arthritis Rheum. 2003; 48:1015-23.
48. Gordon K, Clinical response to adalimumab treatment in patients with moderate to severe psoriasis: Double-blind, randomized controlled trial and open-label extension study. J Am Acad Dermatol. 2006;55: 598-606.
49. Krueger JG. The inmunilogic basis for de treatmen of psorisis with new biologic agents. J Am Acad Dermatol. 2002; 46:1-23
50. Lebwoh M, Menter A. combination therapy to treat moderate to severe psoriasis. J Am Acad Dermatol.2004; 50: 416 - 30.
51. Mease P, Menter A. Quality of life issues in psoriasis and psoriatic arthritis: outcome measures and therapies from a dermatologycal perspective. J Am Acad Dermatol.2006;54: 685-704.
52. Smith CH, Anstey AV, et al. British Association of Dermatologists guidelines for use of biological interventions in psoriasis 2005. Br J Dermatol. 2005; 153: 486-97.
53. Reich K, Nestle F, Papp A, et al. Infl iximad indcution and maintenace therapy for moderate to severe psoriasis: a fase III multicentre double blind trial. Lancet. 2005; 366: 1367-74.
54. Greves J Nunley, et al. Off label uses of biologics in dermatology: rituximad, omalizumad infl iximad, etarnecerpt, adalimumad, efalizumad and alafacept. J Am Acad Dermatol. 2007; 56: e55-79.
55. Sterry W, Barker J, et al. Biological therapies in the systemic management of psoriasis: International Consensus Conference Br J Dermatol. 2004; 151 (Suppl 69):3-17.
Cómo citar
Descargas
Descargas
Publicado
Cómo citar
Número
Sección

| Estadísticas de artículo | |
|---|---|
| Vistas de resúmenes | |
| Vistas de PDF | |
| Descargas de PDF | |
| Vistas de HTML | |
| Otras vistas | |